Shoulder Joint Pain Common Complaints
Many patients present with shoulder joint pain symptoms that frequently reflect referral from the cervical spine i.e. cervical spondylosis.
Symptoms such as trapezial muscle discomfort and upper anterior shoulder pain may have an underlying nerve component.
Clinical examination of the upper limb must involve primary cervical spine assessment looking for areas of tenderness and possible nerve referral.
There may be brachioplexus sensitisation.
Shoulder joint instability usually occurs as a consequence of traumatic injury to the anterior shoulder soft tissues resulting in a labral tear and possible Bankart lesion. This encompasses a small avulsion of the anterior glenoid anterior bone lip. Invariably this is a sports-related contact injury.
At may result in either subluxation which is partial dislocation or complete dislocation of the shoulder joint necessitating manual reduction under anaesthetic. X-rays may show a Hill-Sachs lesion which is better demonstrated on CT or MRI. This is an impaction fracture of the humeral head as it dislocates off the glenoid edge. It may aggravate instability by reducing the surface area.
Soft tissue Remplissage is a treatment option. Occasionally, reverse Hill-Sachs lesions are seen in posterior instability.

In the early stages, conservative treatment with muscle strengthening exercises may suffice to prevent further instability.
If continued perceived instability persists, patients will present with deep anterior pain and a sense of instability centred on the anterior shoulder.
Clinical examination will demonstrate a positive apprehension test on external rotation. The shoulder may in fact sublux forward. Diagnostic investigations include MRI arthrography and/or arthroscopy with arthroscopic labral repair and/or Bankart stabilisation.
Patients will wear a protective sling for a few weeks and undergo supervised physiotherapy not returning to contact sport for between 6 and 8 months. If there is a persistent instability, a Laterjet bone stabilisation procedure may be recommended.
In a small number of patients who have chronic recurrent dislocation, an anterior open soft tissue stabilisation would be recommended.
Frozen shoulder/adhesive capsulitis is a description of soft tissue inflammation of the shoulder joint synovial lining.
It is frequently idiopathic and open associated with underlying neuropathic pain.
It sometimes is associated with trauma, inflammatory nodes or breast disease.
It is more common in females and manifests as severe shoulder pain leading to restriction in movement and progressive stiffness involving over several months.
In the early stage shoulder injection may help with intensive physiotherapy.
If the shoulder becomes frozen, an expectant approach of graduated recovery or alternatively manipulation under anaesthetic and arthroscopic hydraulic distension can be very effective.

Rotator cuff impingement is perhaps the most common shoulder joint pain complaint in the middle aged group.
It manifests as pain on bringing the arm out sideways in abduction past 90° associated with discomfort radiating to the deltoid muscle and particularly present at night-time.
It is often provoked by lifting the arm above shoulder level and precipitated frequently by heavy manual activities.
It may occur following a fall. Acromioclavicular arthritis is commonly present causing mechanical interference.
The biceps tendon may undergo simultaneous attritional changes causing focal pain necessitating bicipital tenotomy or tenodesis.
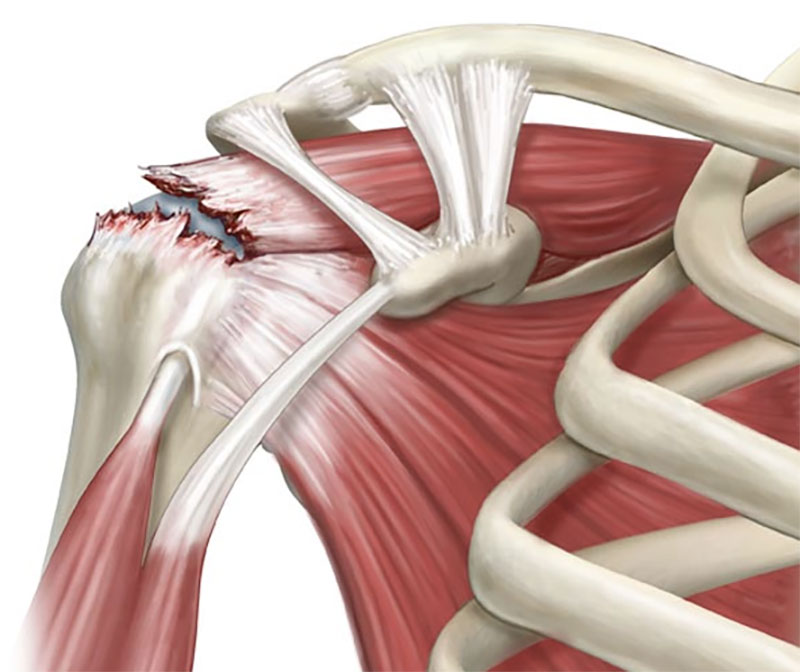
The underlying rotator cuff muscle will undergo attritional tear progressing to a full-thickness supraspinatous cuff tear.
This may be treated in the very low demand elderly patient by injection and physiotherapy.
In the younger patient suffering from shoulder joint pain, arthroscopic rotator cuff repair will be offered.
Patients will wear a protective collar and cuff for a few weeks afterwards and attend supervised physiotherapy/water-based rehabilitation.
In a very small number of patients with completely deficient rotator cuff tears, superior capsular repair incorporating synthetic materials is now becoming available.
An alternative option, is reversed glenohumeral shoulder replacement.

Shoulder joint arthritis is seen in the age group 60 years plus and is far less common compared to other large joint arthritis.
It frequently creates a pseudo-frozen shoulder with mechanical rotation restriction and pain.
Treatment options will include glenohumeral joint replacement in the well-established case provided the rotator cuff is intact. If the rotator cuff is chronically torn, reverse glenohumeral joint replacement will be offered or possibly a superior capsular repair as part of the shoulder joint replacement.
Patients will mobilise in a protective sling for a few weeks and attend supervised physiotherapy.
Isolated symptomatic acromioclavicular joint arthritis may require treatment by arthroscopic subacromial decompression or excising 1 cm clavicle via open mini incision.